IBS or IBD? Irritable Differences of the Bowels
Guadalupe Chavez, PharmD Candidate 2021,
University of Iowa College of Pharmacy
February 16, 2021

Healthy bowel movement frequency can range from three times a day to three times a week. If you or a loved one experience a periodic increase or decrease in stool form or frequency accompanied by diarrhea, constipation, abdominal pain, bloating, or blood in stool that is not normal.
You don’t have to live with these symptoms in silence. Visit your doctor and they may refer you to a gastrointestinal (gut) specialist. Below we will discuss two out of many other bowel disorders, Inflammatory Bowel Disease (IBD) and Irritable Bowel Syndrome (IBS).
What is the difference between IBD and IBS?
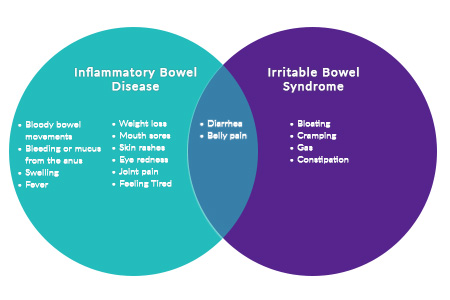
IBD is a term used to describe a group of disorders that inflame parts of the gut. Two major IBD disorders are Crohn’s Disease (CD) and Ulcerative Colitis (UC). While CD causes destructive inflammation anywhere between your mouth and anus, UC primarily effects the colon. Additionally, there is an increased risk for colon cancer in IBD.
IBS is another type of bowel disorder but is a syndrome and not a disease. It should not be confused with IBD. IBS is less severe because there is no inflammation or permanent harm to the intestines. Contrary to IBD, there is no increased risk for colon cancer in IBS.
Because symptoms of IBD, IBS, and other common gut disorders overlap, specialists may order a combination of tests and procedures with the goal to obtain an accurate diagnosis. The average age onset of IBD or IBS is 15 to 30 years of age, but it can present at any age. Because IBD and IBS are not curable, the main goals of treatment are to control symptoms and prevent them from returning.
What are the symptoms of IBD and IBS?
Talk to your doctor or a trusted healthcare professional if you or a loved one experiences these symptoms:
What can I do on my own to feel better?
For IBD and IBS, doctors recommend eating smaller, more frequent meals, staying hydrated, and cutting down on food that make your symptoms worse. Some common foods that worsen symptoms are fruits, vegetables, cheese, yogurt, or milk. Because everyone is different it is best to keep a diary of the foods that make you feel uncomfortable and avoid them. Staying away from medications that worsen your symptoms is also recommended (ie. Ibuprofen, naproxen).
Probiotics may help reduce abdominal pain, bloating, constipation, or diarrhea in some patients. Studies have demonstrated that probiotic species given in combination or alone (ie. Lactobacillus and Bifidobacterium) have the best efficacy evidence for inflammatory bowel diseases.
What if I can’t control my symptoms on my own?
In mild to moderate cases of IBD, doctors may prescribe topical or oral medicine to help reduce swelling. In more severe cases of IBD, medicines that work on the immune system or surgery may be needed. IBS, on the other hand, can be managed with antidiarrheals, laxatives, or antispasmodics if diet modification and supplements alone cannot treat symptoms. In either case, close monitoring by your healthcare provider of treatments is necessary as not all agents are safe in all disorders.
References:
Colombel JF, Shin A, Gibson PR. AGA Clinical Practice Update on Functional Gastrointestinal Symptoms in Patients With Inflammatory Bowel Disease: Expert Review. Clin Gastroenterol Hepatol. 2019 Feb;17(3):380-390.e1. doi: 10.1016/j.cgh.2018.08.001. Epub 2018 Aug 9. PMID: 30099108; PMCID: PMC6581193.
World Gastroenterology Organization Global Guidelines: Inflammatory Bowel Disease. Updated 2015. https://www.worldgastroenterology.org/guidelines/global-guidelines/inflammatory-bowel-disease-ibd/inflammatory-bowel-disease-ibd-english (accessed 2021 Jan 1)
Peppercorn M, et al. Definition, epidemiology, and risk factors for inflammatory bowel disease in adults. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (Accessed on January 13, 2021.)
American College of Gastroenterology (ACG) Clinical Guidelines: Management of Crohn’s Disease in Adults. Am J Gastroenterol 2018; 113:481-517
American Gastroenterological Association (AGA) Clinical Practice Guidelines on the Management of Mild-to-Moderate Ulcerative Colitis. Gastroenterology 2019; 156: 748-764

Save on the Go
For your convenience, use the ScriptSave®WellRx mobile app. Now savings are well in hand, right at the pharmacy counter. Save on your family's prescription medicines.



Get a Prescription Discount Card
Your choice. Get a ScriptSave WellRx Savings Card. Or Download the free mobile app from the App Store or Google Play Store

Grocery Guidance
ScriptSave WellRx Grocery Guidance leverages leading-edge nutritional data science to help you know which food products on your grocery store shelf are truly good for YOU.
Recommended Articles
Desoxyn vs Vyvanse: ADHD Drugs Compared
July 15, 2026
Desoxyn vs Vyvanse compared. Read about the differences in benefits, side effects, dosages, and effectiveness of these two common ADHD medications.

Wegovy Shortage Resolved: 2026 Availability and Pill Launch
July 01, 2026
Is the Wegovy shortage over? Learn about 2026 availability, supply updates, and the latest news on a potential Wegovy pill alternative.

Zepbound vs Ozempic
June 24, 2026
ZepBound vs Ozempic: Understand key differences in results, safety, accessibility, and cost and choose the best medical weight-loss treatment.

